



Search results
After 739 duplicates were excluded, the literature search resulted in 1740 citations. Screening of titles and abstracts excluded 1607 articles, leaving 133 eligible for full-text review. Following full-text review, 38 articles were included in the study. Primary reasons for exclusion of 95 sources at full-text screening included 57 that were the wrong intervention (not focused on school health promotion), 22 that only reported on outcomes, 5 that were a secondary source, 3 that were not available in English, 3 that only comprised an abstract, 3 that included the wrong population, and 2 that were in the wrong setting.
No new sources were identified from reviewing the first 50 pages of Google Scholar. Thirty-five sources were identified from the reference searching, but after review, only 2 new sources were identified. Twelve grey literature sources were identified from related websites, and after review 7 were included. A list of websites searched can be found in Additional File 4. Three further sources were added based on expert opinion. See Fig. 1 for the PRISMA-ScR flow diagram of search results, source selection and inclusion process [31].
In summary, there were 50 sources included in the review. Additional File 5 summarizes key source information included.
Demographics of included sources
Of the 50 sources included in the review, all were published between 2000 and 2023. Over half the studies were from European institutions/organizations (n = 26) [9, 17, 22, 23, 39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60] followed by North America (n = 18) [14, 15, 24,25,26, 61,62,63,64,65,66,67,68,69,70,71,72]. A small number of studies were published in other parts of the world including Asia, Africa, Australia and South America (n = 6) [73,74,75,76,77,78]. Most studies were primary studies (n = 34) [9, 14, 15, 17, 24, 39,40,, 40, 42, 43, 45,46,47,48,49, 51,52,53, 55,56,57,58,59, 62,63,64, 67, 71,72,73,74,75,76,77, 79], while other sources included were commentaries (n = 6) [22, 41, 44, 50, 54, 61], evidence syntheses (n = 3) [26, 60, 78] and grey literature (n = 7) [23, 25, 65, 66, 68,69,70].
Of the primary studies, most involved only student participants (n = 18) [14, 24, 39, 43, 45,46,47, 49, 55, 57, 60, 63, 67, 71,72,73,74, 77] from a range of school levels including elementary (n = 11) [39, 43, 46, 49, 51, 52, 57, 64, 72, 75, 79], middle (n = 3) [40, 45, 55], high school (n = 3) [62, 66, 73] and combined (n = 13) [15, 40, 48, 50, 55, 58, 62, 63, 66, 67, 73, 76, 77]. Twenty sources reported on sex/gender of the participants [15, 22, 40,41,42,43, 47,48,49, 51, 59, 62, 64, 66, 71, 73,74,75, 77, 79], 17 reported on socio-racial status of the participants (e.g. race/ethnicity, socio-economic level of participants/setting) [14, 15, 40, 45, 46, 49, 57, 59, 62,63,64, 66, 71, 73, 75, 77, 79], and 12 reported on if the school was in a rural or urban setting [15–47, 49, 57, 64, 66, 67, 72, 74, 75, 77].
Most sources in the study used qualitative designs (n = 28) [9, 14, 23, 24, 39,40,41,42, 45,46,47,48, 52, 55, 56, 58, 62, 64, 66, 67, 72,73,74,75,76,77, 79], while other sources used mixed- or multi- methods (n = 7) [15, 49, 53, 57, 58, 63, 65], quantitative (n = 3) [43, 51, 71], or evidence synthesis designs (n = 3) [26, 60, 78]. Qualitative methods used included interviews (n = 22) [9, 14, 15, 17, 40, 41, 48, 53, 55, 57,58,59, 63, 64, 67, 72, 74,75,76,77, 79], focus groups (n = 21) [14, 15, 24, 39, 40, 42, 47,48,49, 52, 53, 58, 59, 62, 63, 65, 72, 73, 75, 76, 79], photovoice (n = 3) [14, 59, 77], observational techniques (n = 9) [17, 45, 55, 58, 64, 66, 72, 75, 79], document review (n = 10) [9, 15, 17, 46, 55, 58,59,60, 62, 66], and reflective activities (n = 4) [52, 59, 66, 77]. Other methods used in the sources also included survey tools (n = 7) [15, 43, 51, 53, 58, 63, 71] and evidence synthesis techniques (n = 3) [26, 60, 78]. The methodological paradigms and approaches ranged in terminology, but largely were associated with a qualitative paradigmatic view with participatory methodologies most frequently reported (n = 19) [14, 23, 24, 39, 41, 46, 48, 51, 52, 55, 59, 62, 66, 67, 71, 72, 75, 77, 79], as well as case study approaches (n = 10) [9, 23, 17, 46, 53, 55, 64, 71, 72, 76]. Table 2 outlines further demographic information on the sources included in the review.
Program/Activity strategies for student engagement in school health promotion
From applicable sources of primary research that outlined programs/activity strategies for student engagement in school health promotion there was a range of content topics with most programs/activities having a broad focus on health (n = 27) [9, 14, 15, 23, 24, 26, 39, 43, 45, 46, 50, 51, 56, 57, 59, 61,62,63, 65, 66, 69,70,71, 73, 74, 77, 79], while other programs/activities focused on food/nutrition (n = 3) [53, 55, 72], physical activity, (n = 2) [42, 49], both food/nutrition and physical activity (n = 3) [17, 47, 64], mental health (n = 3) [40, 48, 58] and disease prevention (n = 1) [76].
Across applicable sources, categories were developed based on the common program/activity strategies to engage students in HPS. Program/activity strategies were regularly outlined in a cycle of engagement that were acknowledged as non-linear and iterative, thus are outlined in no particular order including: (1) Co-development between adults and students, (2) Opportunity to reflect and envision health concepts, (3) Developing and determining priorities through inquiry, (4) Action-oriented learning, and (5) Alignment with school focus.
An overarching category was the use of participatory approaches to enhance meaningful and collaborative engagement of students in school health promotion. This overarching concept was apparent in each of the outlined categories such that student voice was intentionally involved in different stages of the process of student engagement in HPS including development, planning and implementation [9, 17, 23, 24, 39, 43, 47, 48, 52, 63, 65, 66, 71]. Of note, eight sources identified the use of the IVAC model (Investigation, Vision, Action, Change) when outlining the program/activity strategies instilled as a guide for student engagement in school health promotion [9, 17, 22, 23, 41, 43, 55, 57]. The IVAC model encompasses various participatory principles identified in other program/activity strategies, but in a more directed manner where children and youth are supported to investigate different health issues that affect them, create visions about desirable changes, and act towards desirable action [43].
-
1)
Co-development between adults and students.
Programs and activities that engaged students in school health promotion widely involved the co-development of projects through shared-decision making between adults and students [9, 17, 23, 24, 46, 47, 51, 58, 66]. This was regularly put into practice through the development of formal or informal committees made up of students and different adult supporters such as teachers, school nurses, administrators, and designated healthcare or health promotion professionals [46, 51, 66]. The collaborative role of the adults in said groups was largely to guide students across a participatory cycle of engagement [9, 17, 24, 48, 51, 58, 61, 62, 76], such as through facilitating group discussions [24] or aiding in data collection and analysis [61]. Adequate training was identified as a necessary component of co-development, such that it is important for both students and staff to be well-equipped with the knowledge and skills needed to meaningfully take on roles related to school health promotion activities and student engagement [24, 47, 57, 58, 62, 71].
-
2)
Opportunity to reflect and envision concepts of health.
A strategy identified across various school health promotion programs and activities involved the opportunity for children and youth to have space and time to reflect and envision their own concepts of health [9, 14, 17, 39, 43, 45, 46, 51, 57, 59, 66, 73]. Many of the programs and activities recognized health as a broad concept that is multidimensional, multidisciplinary and a collection of personal, social and environmental connections [9, 15, 17, 23, 43, 51, 55, 57,58,59, 62, 73]. Thus, this ideology translated into programs/activities that provided the opportunity for students to subjectively develop their own perceptions of health through personal and collective experiences with peers [39, 45]. Methods to evoke reflection and visions of health included reflective writing [73], facilitated dialogue [24, 39], and taking and interpreting photos of the school health environment [14, 59].
-
3)
Developing and determining priorities through inquiry.
An additional strategy noted in various school health promotion programs and activities involved students assessing their individual and school health needs and further developing priorities based on their inquiry [17, 24, 40, 46, 53, 57, 59, 62, 66, 71]. Priority decision making involved acts of strategic planning, expressions of needs and deciding on issues affecting their lives through different data collection and analysis techniques [14, 23, 24, 40, 49, 52, 58, 59, 61, 63, 66, 71]. Involving students in inquiry allows them to further examine the health needs of their peers and/or wider school community [40, 58, 64, 66, 71], as well as increases their ownership through understanding of their own health data [24]. Methods executed in the sources included employing needs assessments and surveys [71], conducting photovoice projects [14, 59, 61] and peer to peer interviews [67].
-
4)
Action-oriented learning.
Action-oriented learning was a key characteristic of engaging and sustaining students in school health promotion programs and activities [9, 17, 23, 24, 39, 41, 43, 46, 53, 57, 66, 71, 72]. In practice, this involved students recognizing the ability to enact change through connecting their reflective, visionary and priority exercises to realistic action in their school health environment [39]. Sources identified that this connection from school health promotion theory to action can be gained through participation in practice-based mechanisms such as presenting their vision, advocating for change and promoting external dialogue on issues of interest [23, 24, 57, 59, 66]. Further, being involved in the operations of actioning ideas such as mobilizing resources or participating in on the ground implementation [53, 65, 66, 72] was essential for students to link vision to change.
-
5)
Alignment of strategies with school focus.
A distinct tactic employed by programs and activities aiming to actively engage students in an initiative or project related to school health promotion was to strategically embed and/or align their objectives with pre-established practices in the school curriculum [17, 45, 47, 49, 51, 55, 62]. For example, this often showed up as embedding health promotion initiatives such as physical health as an ongoing part of different school classes including math or language arts [49, 51] or attaching a certain health promotion program or project to a pre-developed health class such as Health Education [55, 57].
Facilitators and barriers to student engagement in school health promotion
Intersecting facilitators and barriers to student engagement in school health promotion were identified at each level of the SEM including individual, interpersonal, and system-level factors. The facilitators and barriers were found to be overlapping; therefore, categories were developed to capture both promoting and hindering factors to the engagement process for contextual purposes including: (1) Student and adult motivation to be involved, (2) Child and youth capability and development, (3) Adult’s approach to engagement, (4) Group dynamics, (5) School structure, and (6) Buy-in and connection from partners with authority. To aid with clarity and deviation of influential factors, facilitators and barriers are further broken down by the SEM in Fig. 2.

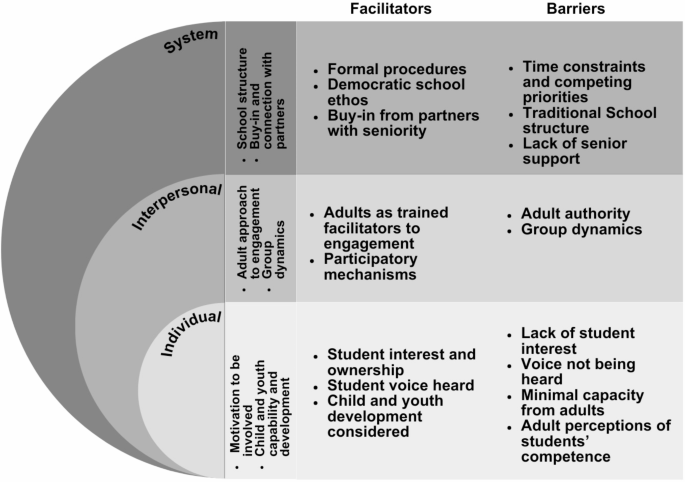
Facilitators and barriers to student engagement in school health promotion categorized by the socio-ecological model (SEM)
Individual-level.
-
1)
Student and adult motivation to be involved: Sources suggested that overall student motivation such as their wants, needs and desires can impact their degree of engagement in school health promotion. Their interest and commitment were found to be either a promoter or deterrent to their involvement and was largely linked to their feeling of ownership [17, 22, 24, 25, 41, 44, 49, 60, 62, 66, 67, 72, 75, 79] or lack thereof [22, 23, 26, 39, 41, 67, 76]. Student ownership was manifested as having their opinions taking seriously [26, 44, 47, 51, 60, 67, 70, 75, 76] versus their voice not being heard [22, 23, 26, 39, 41, 67, 76]. Student involvement in understanding their own data can heighten the ownership process [48], as well as peer-to-peer support [15, 40, 41, 44, 46, 47, 64, 70, 72, 73, 75, 79] such as dialogue and collaboration between pupils and student mentoring. In relation to adults, the capacity to be actively involved in engagement practices is a limitation, such as the energy it takes to meaningfully facilitate and support students, as well as the commitment to long-term reform [23, 53, 61, 62].
-
2)
Child and youth capability and development: It was recognized from the sources that a facilitator to engagement was when adults recognize student capability and consider their level of cognitive development to be of value, rather than a limitation to engagement [25, 26, 54, 61, 62]. In practice, this translates to a scaffolding approach where adults meet students where they are at through youth friendly materials [25, 79] or use of methods consistent with the development of logical reasoning [61]. By contrast, a barrier noted was the pre-conceived attitudes and perceptions that adults can hold regarding the limited capability and competence students need to be actively engaged in school health promotion [23, 25, 41, 45, 50, 54, 59, 61, 72, 76]. These perceptions can lead to adults adapting what is ‘appropriate’ to teach in class [45] or limiting engagement opportunities for students [41, 72]. As stated by Vanner et al. [72, p. 342] engagement is often viewed as an “instrumental perspective of participation rather than a child rights conception,” leading to tokenistic rather than genuine involvement [41, 72].
Interpersonal-level
-
3)
Adult’s approach to engagement: The practical approaches taken by adults to engage students in school health promotion have considerable impact on promoting or hindering engagement. Adults who approach engagement through the role of a facilitator such as supporting, guiding and encouraging student voice can enhance the engagement process, rather than top-down teaching mechanisms [15, 23, 40, 44, 67, 71, 73, 79]. This form of support was referenced as adults being open-minded to collaborate with students [9, 26, 40, 54, 60,61,62, 79], build trusting relationships [14, 25, 40, 41, 61, 74, 77, 79], encourage students to participate [15, 40, 44, 67, 73], and applying participatory mechanisms [9, 17, 24, 39, 46, 51, 66, 70]. The practice of participatory mechanisms largely related to the use of experiential learning to actively engage students with their peers and the social/physical health environment [17, 24, 40, 43, 49, 64, 73, 75, 76] such as ‘learning by doing’ [75] and practice-based activities [49]. However, it was also identified that for adults to engage students adequately and appropriately, they must have the capability to do so through capacity building and training opportunities [17, 22, 44, 59, 60, 72,73,74,75].
Approaches to engagement that mimicked authoritative and hierarchal practices negatively impacted the process of student engagement in school health promotion. This includes the act of adults driving decisions [53, 59, 62, 69, 77] such as monopolizing discussions [62] and a lack of shared decision-making with students [9, 17, 48, 59, 62]. The sources also identified that adults can feel a ‘loss of control’ during more collaborative practices; thereby further inhibiting meaningful engagement with students [25, 44, 75, 76].
-
4)
Group dynamics: Group dynamics mainly related to the structure of a formal or informal group or committee influencing the engagement of students in school health promotion. Composition of the group including diversity, and number of students as well democratic election processes, if applicable, impacted the level of engagement [55, 60, 61, 67, 75]. For example, larger group sizes were viewed as a barrier to engagement practices [55, 61, 75]. Further, lack of clarity about student/adult roles were shown to impact engagement [15, 48, 58], such as what responsibilities were expected of the students versus adults in facilitating activities and leading tasks [48, 58, 60]. This confusion also impacted relationship dynamics between students and adults such as power relations and ability to collaborate [17, 48, 59, 62]. Of example, adults have more focus on outcome measures compared to students, a phenomenon which can inadvertently impact the participatory process [17, 48].
System-level
-
5)
School structure: The structure of the school such as its overall culture, ethos and policies impacts the engagement of students in school health promotion. It was acknowledged by sources that schools which promote democratic, reflective and supportive practices enable authentic participation of students [17, 22, 54, 60, 61, 75, 78]. Examples related to this ideology include collaborative dialogue between students and teachers, rather than imposing participation of a task on a student [22], as well as providing a system of support for adults to build capacity in HPS and participatory approaches [78]. It was also recognized in the sources that an enabling factor is if organizational principles and beliefs are formalized into regulated or guiding policies on student engagement in HPS. Examples include developing structured timelines, formal development of action teams, building boundaries of roles/responsibilities for student and adult partners (e.g. terms of reference), and clearly defining the importance of student voice in administrative documents related to school health promotion [40, 53,54,55, 60, 62, 71, 72, 78, 79].
By contrast, a number of sources highlighted that a school’s more traditional and historical focus on a structured and controlled environment was not conducive to meaningful engagement in school health promotion [17, 22, 23, 39, 45, 61, 62, 65, 75]. Of note, traditional teaching methods that centre students as recipients of information, rather than reflectors or producers of knowledge, was identified as a barrier [14, 17, 22, 41, 45, 54, 59, 62, 65] such as maintaining students in their role as pupils and “subordinates” to teachers [39, p. 25]. In relation to school health promotion, this involves students being taught and made to accept pre-existing health ideologies of what is determined ‘healthy’ or not, versus open dialogue and reflection on what they believe to be related to their health and well-being [54]. The value and pressure placed on improvement outcomes such as academic achievement practices [9, 15, 45, 62] were also acknowledged to detract from student engagement in school health promotion practices. Lastly, time constraints due to competing priorities of the traditional school structure such as extracurriculars, an overloaded curriculum, and administrative duties [15, 17, 23, 26, 45, 50, 53, 58, 61,62,63, 65, 71, 72, 75, 76] also served as a barrier to engagement.
-
6)
Buy-in and connection with partners with authority: Buy-in and connection with partners who have authority [17, 23, 24, 40, 58, 60, 69, 71] or lack of [17, 40, 59, 62] was noted as both a facilitator and barrier to student engagement in school health promotion. Enabling factors focused on the support of senior management [58] or principals [40] who had the ‘power’ to change wider policies and action change, while mitigating factors related to absence of senior management and partners within and beyond the school. Lack of system-level support involved absence of formal agreements, as well as minimal connection to decision-makers, or external community members who could influence the engagement process [17, 40, 59, 62].
Form of student engagement
Applicable sources (n = 35) ranged in their forms of engagement with most sources (n = 30, 86%) being categorized as Level 3 or higher (Fig. 3). Few sources were categorized at Level 2 (n = 5, 14%) [42, 48, 72, 73, 76] and none at Level 1. Author reasoning for categorization into specific levels of engagement can be viewed in Additional File 6.

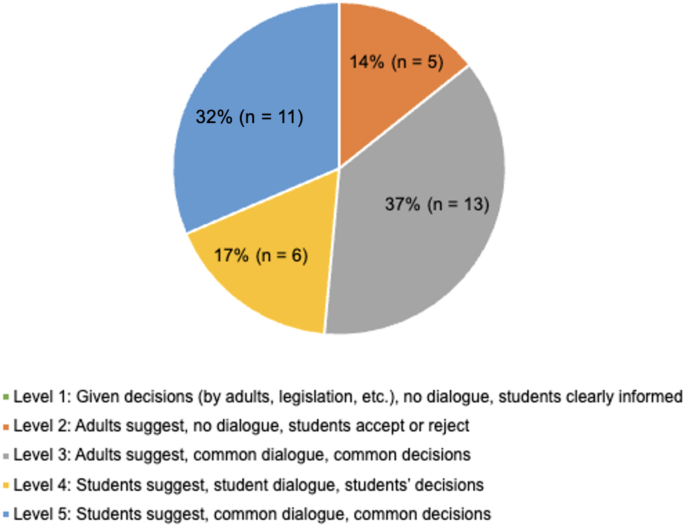
Forms of student engagement adapted from Jensen and Simovska [22]
Outcomes of student engagement in school health promotion
As a secondary information, outcomes were included and categorized per SEM level if reported in the sources. Of the outcomes identified for engagement of students in school health promotion programs/activities, a large number of factors were reported at the individual level including enhancing student health and well-being [15, 22, 25, 43, 47, 51, 58, 73, 76], advancing personal development skills [8, 14,15,16,17, 25, 44, 47, 48, 50, 51, 54, 61, 62, 64, 66, 76], increasing student participation [15, 44, 47, 49,50,51, 56,57,58,59, 61, 72, 73, 77], and improving student perceptions of schools [39, 40, 43, 45, 46]. At the interpersonal level, positive peer to peer relationships were identified [9, 25, 59, 71], as well as student-adult relationships including student to teacher [25, 54, 60, 71] and student to health professional [66, 74]. Lastly, at the system-level various positive outcomes were highlighted including supporting a healthier school environment [17, 22, 39, 59, 60, 72], aiding in better health services for student’s needs [71, 74] and student-centered policies at the school level [17, 22, 25, 40, 60].
link