Regulation of health professions education and the growth of schools in Somalia | BMC Medical Education

Proliferation of medical schools
This study identified 112 health professions schools across Somalia (S1) with varying distributions among different states. Approximately 54% of these institutions are in Benadir state, reflecting the concentration of educational resources in urban areas. However, schools have also been established in other states, such as Somaliland (20%), Puntland (8%), southwest (8%), Galmudug (4%), Hirshabelle (4%), and Jubaland (3%). Figure 1 shows the growth of schools in Somalia over time, with their establishment years ranging from 1969 to 2023. A significant number of these schools have been established over the last decade, highlighting a recent surge in the proliferation of medical schools. Figure 2 provides a geographical representation of the distribution of the schools in Somalia. The map is marked with red dots representing 25 schools listed in the World Directory of Medical Schools and blue dots representing those that are not listed in the directory.
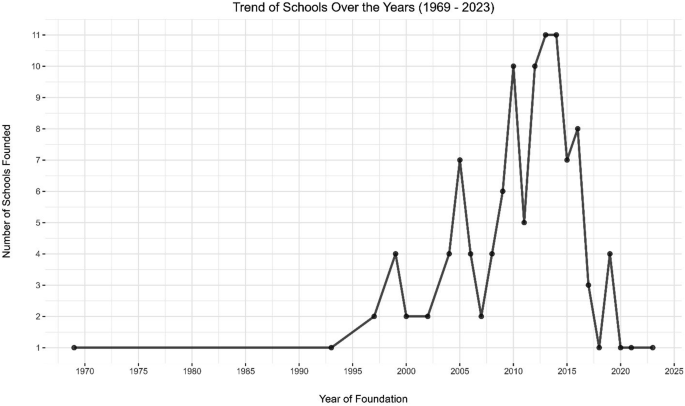
Trends in schools founded over the years (1969–2023)

Distribution of health professions schools across different states in Somalia
Health workforce assessment
This study evaluated the health workforce across the Benadir Regional Administration (BRA) and the states of Galmudug, Hirshabelle, Jubaland, Puntland, and Southwest. A total of 13,236 health professionals were identified, with 7,073 (53.4%) comprising of physicians, nurses, and midwives. The remaining included medical laboratory technicians, pharmacists, and public health officers. This workforce density falls below the World Health Organization (WHO) lower threshold of 2.3 skilled health professionals per 1,000 people, estimated for a population of 13 million. The distribution exhibits a pronounced urban-rural disparity, with significant shortages in both rural areas and larger urban centers at the federal and state levels. This imbalance underscores the need for targeted interventions to ensure equitable access to healthcare services across all regions in Somalia.
The physicians interviewed found their educational programs productive, especially through university partnerships with public and private hospitals in Mogadishu and month-long community medicine experiences in rural areas. However, they noted the incoherence of existing healthcare rules and regulations as well as the lack of recruitment and employment standards in these hospitals, both in the management of service providers and patients. The ratio of physicians to nurses and midwives is 1:5, compared to many African countries where the ratio is similar, and developed countries where it is closer to 1:3. This emphasizes the significant contribution of nurses and midwives to the health care system.
Figure 3 highlights the disparities in the distribution of health professionals, showing the Benadir Regional Administration (BRA) with a substantial concentration of health workers: 668 physicians, 401 midwives, and 1,438 nurses. In contrast, Galmudug, Hirshabelle, and Jubaland had markedly fewer health professionals, suggesting limited healthcare service accessibility. Puntland and Southwest are moderately staffed, with Puntland having 210 physicians and 425 midwives and Southwest having 96 physicians and 398 midwives. The number of nurses was similar in both regions, with 775 in Puntland and 743 in the Southwest. Table 1 illustrates the deficits of physicians, nurses, and midwives in various levels of the health system. According to the minimum WHO staffing threshold of 23 professionals per 10,000 people, there is a requirement for 30,000 such professionals, representing a shortfall of 20,793 individuals.

Regional Distribution of Health Professionals. (Source: Ministry of Health’s HRH report (2021)
In the second scenario, adopting the WHO’s preferred density rate of 44.5 professionals per 10,000 population, the need escalates to approximately 57,850 health workers, resulting in a gap of nearly 48,500. The inability of the health sector to employ all necessary graduate health workforce categories exacerbates this shortage. Despite the annual graduation of physicians, nurses, and midwives, employment opportunities remain scarce in both the public and private sectors, indicating a pressing need for policy review in health sector financing by the public sector.
Focus group discussion with young physicians
The physicians interviewed expressed dissatisfaction with employment opportunities after graduation, highlighting the need for strong connections and family linkages to secure jobs. One participant stated, ‘Without connections, it is almost impossible to find a decent job in the healthcare sector.’ This sentiment was echoed by others, who noted a lack of fair recruitment practices. Another interviewee remarked, ‘Most of my colleagues who got jobs had some form of connection within hospital administration.
Physicians indicated that the private sector is equally affected by the need for strong connections and family linkages for job offers. On many occasions, the only opportunity offered is voluntary practice without financial compensation, which many accept as advancing their professional skills. This makes the private sector less attractive. One participant jointly established a small clinic with a fellow physician, and said that they were managed reasonably. However, his colleagues indicated that this avenue of employment is only possible for a limited number of people who can afford the upfront tangible investment for establishing a clinic.
The physicians interviewed felt that the above reasons severely limited their professional opportunities, in many cases compelling graduates to change their profession and engage in non-health areas or opt for a life as a housewife, as is the case for many female health professionals.
Employment and education perception survey
In less than two weeks, 388 students from across the country responded, demonstrating their interest in regulations. After excluding 35 responses from non-health-related fields, we analyzed data from 353 students, most of whom were enrolled in priority courses, such as nursing (33%), Public Health (22%), Medicine and Surgery (15%), midwifery (14%), and medical laboratories (10%). Approximately 80% of respondents were satisfied with the quality of their training. However, 56% of the students from the BRA who responded were dissatisfied. About 70% of students would prefer to study in Somalia, thus building the case for standardization of academic training experiences across the country.
In contrast with the practicing physicians interviewed, almost 90% of the students perceived their employment opportunities to be good, and 80% agreed to consider working in rural areas if given a chance. Close to 30% of BRA and 15% of Jubaland students do not consider their employment opportunities to be good. However, all agreed that the existing workforce demanded more opportunities for practical training, professional development, employment, and stricter regulations. Several challenges in working in rural areas, dominated by a lack of security and terrorism, were highlighted.
Insufficient HRH team capacity for regulatory functions
Interviewees described that the HRH team’s capacity at both federal and state levels was insufficient to carry out all the regulatory and non-regulatory activities required. At both the federal and state levels, there are not enough workers in teams. In addition, many HRH team members do not receive the necessary training to perform their work optimally. Most teams have little budget beyond their salaries, meaning that there is little or no budget for communication, printing, travel, IT, or training.
Regulatory framework
The interviewees stated that the insufficiency of a functional health regulatory framework was a challenge in establishing medical regulations. They described the institution of a health regulatory framework as an important milestone in standardizing professional health education in both pre-service and in-service training and practice. Interviewees described that, in the absence of a formal regulatory framework during the past decades, loose self-regulation has been the norm. Several professional groups, including medical and dental associations, nursing and midwifery associations, pharmacists, and other professional groups, have organized their members to improve access to and quality of healthcare services, set standards of best practice, promote health, prevent diseases, and deliver curative and rehabilitative services following the established health sector service delivery guidelines.
These associations were also formed to protect and guard their respective professional interests in terms of regulation, licensing, Continuing Medical Education (CME), continuing professional development (CPD), preserving ethical norms, setting practice standards, and representing their professions at the national and international levels. In the absence of a binding national or state-level regulatory framework, professional associations sustained a voluntary registration system with weak licensing authorities, while having little or no influence on the pre-service regulation of their respective educational institutions.
Lack of licensing exams
Interviewees stated that credentials obtained from educational institutions act as proxy licensing permits, enabling new graduates to seek employment opportunities in the healthcare system. Neither the educational institutions nor the health facilities that would potentially employ these newly graduated professionals are registered or licensed, although most educational institutions are voluntarily registered by the Ministries of Higher Education and/or by competent state-level government authorities where they operate formally.
Lack of continuing professional development
This study found a significant gap in the professional development of health workers in Somalia, with no existing mandates for Continuing Professional Development (CPD). This lack of CPD requirements is further compounded by the general scarcity of training opportunities, which hinder the ongoing enhancement of skills and knowledge among health professionals. However, the introduction of the National Health Professionals’ Council (NHPC) Act marks a pivotal change, acknowledging the importance of CPD for the entire health workforce. This recognition by the NHPC paves the way for implementing structured CPD programs that are essential for maintaining high standards of care and ensuring that proficient and up-to-date professionals deliver health services.
Lack of accreditation of Pre-service Education (PSE)
School representatives and federal and state representatives generally agreed that the federal government, in close collaboration with the states, should accredit pre-service education for the five main cadres (physicians, nurses, midwives, pharmacists, and dentists), and that the states should accredit pre-service education for all other cadres. There was agreement on the need to harmonize all other cadres across the states to allow health worker movement and avoid confusion. The schools indicated that they were mainly self-regulating and tended to have little contact with either the Ministry of Health or Ministry of Education. The schools mentioned that regulatory uncertainty made it difficult to establish new schools and expand the existing programs. It was also stated that because there were no set standards for the length of training or competencies for each cadre, the competencies of graduates of a given profession differed greatly from school to school, creating uncertainty in the labor market.
Professional misconduct and disciplinary powers
Interviews with key informants revealed a prevalent issue of misconduct involving individuals known as charlatans. Charlatans falsely present themselves as licensed health workers, particularly physicians and pharmacists, despite the lack of official credentials. Key informants generally recognized dual practices, wherein health workers employed in public institutions also operate private practices, as widespread and not considered problematic. In the Somali health system, dual practices help health workers supplement their low public salaries and maintain public employment.
link






